Haemophilia Liberation?
Last week I commenced my haematology rotation at the Royal Children's Hospital, of which one of the highlights so far was an opportunity to observe the outpatient haemophilia clinic.
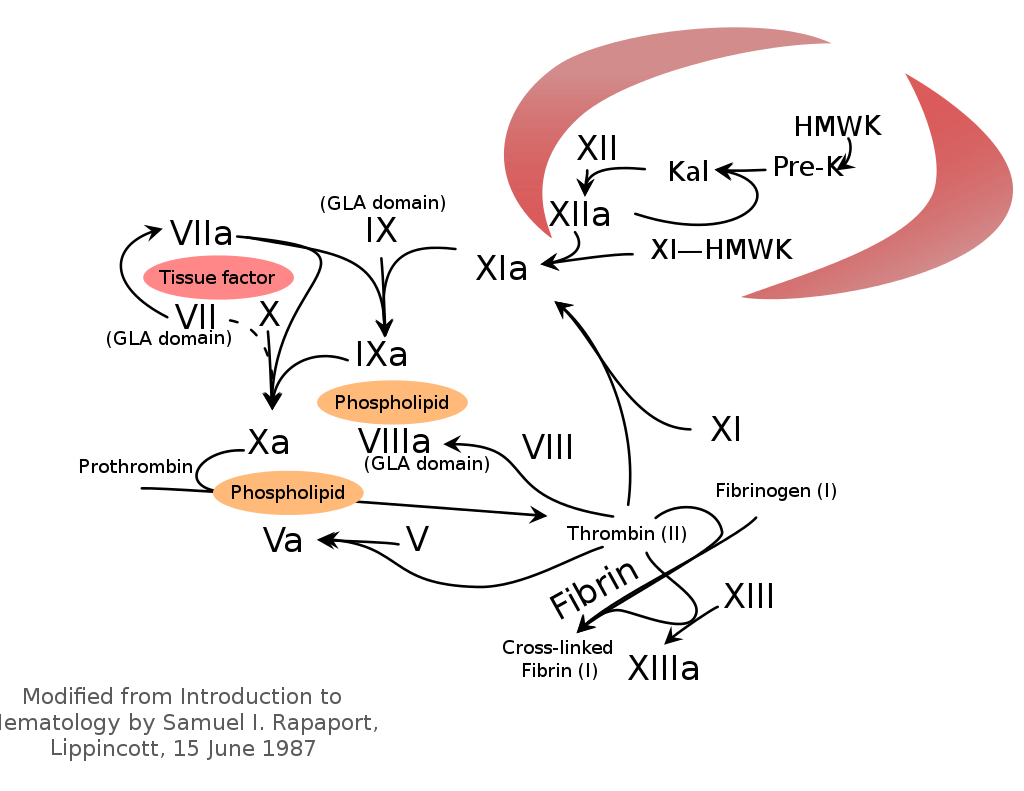
But before that, a bit of background. Haemophilia is a coagulopathy that comes in two types, A and B, which correspond to deficiencies in Factors VIII and IX respectively. These factors, being key enzymes in the coagulation cascade, are activated in the event of a trigger; they in turn activate Factor X, eventually leading to fibrin clots. Deficiencies in these factors increase bleeding risk, especially in places you really don't want to have blood (eg. muscles and joints). Severe bleeding can be life-threatening.
Both haemophilias are usually inherited in an X-linked recessive pattern (and so almost always affect boys). Haemophilia is probably the most famous inherited disease, as its place in the public consciousness is cemented as the "royal disease" that plagued 19th-century Europe's royal houses. Out of these royals, the most unfortunate would probably be Alexei Romanov, the last crown prince of Russia, whose debilitating haemophilia worried his parents so much they engaged the notorious Rasputin for his faith-healing. This relationship was so scandalous that it severely damaged the royal family's popularity, which contributed to Imperial Russia's collapse into revolution.
In Alexei's day, there was no cure for haemophilia; treatment consisted of months-long bed rest after a minor bump. Luckily, medicine progresses. Blood plasma transfusions gave way to cryoprecipitate (a spun-down plasma) in the 20th century, which in turn was superceded by recombinant (lab-grown) factors.
There were a few problems. Firstly, regular factor transfusion as prophylaxis is a major burden, with patients likely requiring 2-3 transfusions every week. Secondly, and more worringly, the transfused factors might provoke an immune response, which destroyes the exogenous factors and renders the whole process useless; this is known as "inhibition". Inhibition rates are high (~30%) in haemophilia A, and these patients require complex management (such as using much larger transfusions, or using other factors such as VIIa to "bypass" the Factor VIII quandry).
This brings me back to the haemophilia clinic. To my surprise, none of the boys who came in that day were receiving factor transfusions! Instead, all the haemophilia A boys were on this drug: emicizumab, or Hemlibra.
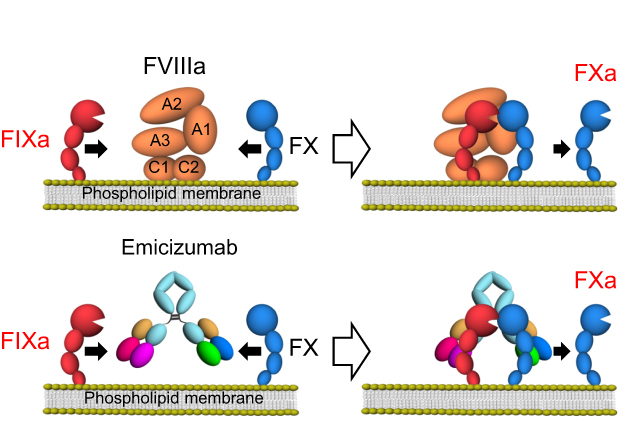
I have never heard of this before, nor were we ever taught about it. That's because it is very very new, having only received TGA and FDA approval in 2018. Emicizumab is a monoclonal antibody binds and activates Factors IX and X, essentially performing the function of the truant Factor VIII. It really did sound like a miracle drug; it apparently is very well tolerated by patients and is incredibly effective as prophylaxis against bleeding. There is minimal risk of inhibiton or clotting. Best of all, in Australia it is provided free of charge (despite being a monoclonal antibody)!
Being such a new drug, current guidelines are rather conservative, requiring an infant to have had at least one bleeding episode to be eligible. However, trials are under way to assess its suitability as a routine prophylaxis for infants. My consultant actually recruited a 3-month bub into a trial for this trial. In his view, emicizumab was such a safe and effective drug that it should not be withheld; hopefully these trials can prove him right.
It really does seem like a very exciting time for haemophilia treatments. A similar monoclonal antibody is in development for haemophilia B. There also exist efforts investigating gene therapy. In any case, I feel that haemophilia is yet another example of human ingenuity triumphing over what was a death sentence a century ago.
Had emicizumab been around in 1904 (Prince Alexei's birth), maybe world history would have gone down a very very different path.
